 |
Jepa Foundations Education and Authentic Development |
||||||||||||||||||
|
|||||||||||||||||||
|
|
Medical Care in Rural municipalities in Guatemala
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| TABLE 1 - COST OF TYPICAL TREATMENTS | ||
TREATMENT |
MUNICIPAL CLINICS, Q | PRIVATE CLINICS* |
Tooth extraction |
65 | 175 |
Cordal surgery |
325 | 500 |
White fillings |
125 | 250 |
Gray fillings |
85 | 175 |
Sealants |
50 | 100 |
Cleaning |
125 | 220 |
Porcelain crowns |
840 | 1.400 |
Acrylic Removable Prosthesis |
600 | 1.200 |
Removable Chrome Prosthesis |
1.500 | 2.000 |
Channels treatments |
300 | 950 |
Total Prosthesis |
900 | 1.800 |
* Average value of 5 private dental clinics located in Antigua Guatemala. Variations are between Ca. ± 30% August 2019. Note: most private clinics do not publish their tariffs (Melsi Simeon.)
Details regarding the organization and performance of the clinics are summarized below.
Santa Catarina Barahona
The clinic was inaugurated in June 2009 under the administration of the Mayor Al Oscar Eliud Gonzales. In 2012, the Mayor Lic. Aftali Ordonez was elected and reappointed for a second term, in 2016. Dr. Eugenia María Eugenia Ramos has been the dentist serving the clinic since its institution on a two days/week basis. In 2014, Dr. Edgard Montes, a maxillofacial specialist who operates a clinic in the Capital City, offered his service at a small charge, on one day/month basis. Typical treatments and applied charges are those included in Table 1. The performance of this clinic, illustrated in Table 2, evidences a steady, yearly increase of the number of patients from Santa Catarina and neighboring towns.
| TABLE 2 - PATIENTS OF SANTA CATARINA BARAHONA | |||
YEAR
|
PATIENTS (total) | SANTA CATARINA BARAHONA | NEIGHBORING TOWN |
2013 |
1.352 | 1.000 | 352 |
2014 |
1.414 | 1.300 | 114 |
2015 |
1.498 | 1.200 | 298 |
2016 |
1.598 | 1.400 | 198 |
2017 |
1.618 | 1.418 | 200 |
2018 |
1.681 | 1.400 | 281 |
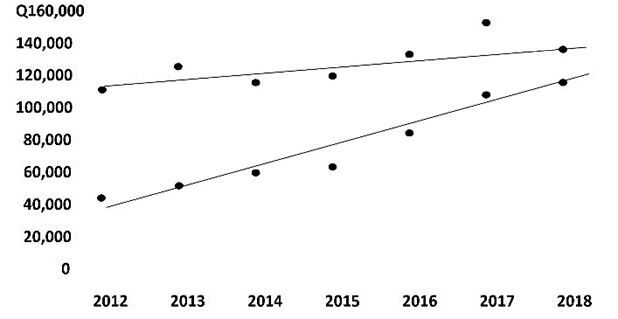
The economic balance of the clinic is illustrated in Table 3 and Figure 1. The data reveal a significant increase over the years of the total earning due to contributions from patients. The total maintenance expenses also increased over the years, but at a reduced rate with respect to the earnings. The two lines in Figure 1 were determined from least square analysis. Their extrapolation reveals crossing in about 2020, when the clinic should become theoretically self-supporting. The clinic, recognizing its mission of public service, does not aim to auto-sustainability. Any eventual surplus will be invested in additional facilities or activities for the benefit of the community, such as an extended time for attention to patients, plans of prevention and visits to families and schools.
| TABLE 3 - YEARLY VARIATION OF INCOME AND EXPENSES | ||
YEAR |
INCOME (quetzales) | EXPENSES (quetzales) |
2012 |
40.000 | 108.123,70 |
2013 |
47.285 | 122.362,19 |
2014 |
55.107,05 | 111.509,87 |
2015 |
58.595 | 115.622,10 |
2016 |
79.592 | 129.241 |
2017 |
103.610 | 148.670,02 |
2018 |
110.565 | 131.399,60 |
| FIG.1 - GRAPH OF TABLE 3 |
The Mayor Neftali Ordonez was reappointed for a third term from 2020 to 2024.
San Miguel Duenas
The second dental clinic was originally planned for inauguration in the Puesto de Salud de San Miguel Dueñas in 2011, under the direction of a tripartite board that included the Foundation, the Municipality and the Ministry of Health. However, the participation of the Ministry had to be withdrawn due to the impossibility of charging in the public structure. The clinic, relocated in the Municipal building, was inaugurated in May 2013 under the administration of Dr. Julius Cesar Quinones who remained charge until December 2015.
Under the Quinone’s administration, the clinic attained high-quality level and patient satisfaction. Regular annual meeting of the Junta with representatives of the Foundation were held. Dr. Quinone supported the individuality of the clinics established w in cooperation with the Foundation. In particular, only patients from Dueñas were attended, appointment were not computerized and a receptionist was not appointed. Moreover, charges to the patients even smaller than those applied in Santa Carina were adopted. Typical examples are included in Table 4.
| TABLE 4 - COST OF TREATMENTS IN THE MUNICIPAL CLINIC OF SAN MIGUEL DUENAS | |
TREATMENT |
FEE (quetzales) |
Extraction |
25 |
White filling |
50 |
Gray filling |
25 |
Sealants |
20 |
Cleaning |
20 |
| Channels treatments | 100 |
Dr. Dinora Ximucane was the dentist hat attended patients five days a week from 8 to 12. The number of patients attended increased considerably during the Quinone administration from May 2013 until December 2013. The gap between income and expenses was considerably larger than in the case of Santa Catarina Barahona (Fig.3) and was covered by the Municipality.
In 2016 a change in the administration of the town occurred. Alejandro Fernandez Carera, the new Mayor, followed the practice of Dr. Quinone regarding the small charges for the treatments, attention limited to Dueñas residents and daily operation from 8 to 12. Annual meetings with representatives of the Foundation were not held. A new experienced dentist, Dr. Benito Guerriero, appointed in 2016, moved to a new position late in 2017. A new young dentist, Dr. Eduardo Franco, was appointed in February 2018. He reports that attendance considerably increased during the three semesters in which he has been in charge, attaining the rate of to about 10 patients a day.
In 2018 an important event occurred. The clinic was transferred to a new location where a structure intended to be a small municipal hospital had been built during the Quinone administration with support from a German Foundation and resources of the Municipality. The Fernandez administration was able to expand the facility into a small medical center that was named Centro Maria Teresa. The following clinics are now operating within the Center:
- Dental Clinic
- Psychology Clinic
- Nutrition Clinic
- General Medicine Clinic
Further additions are planned. In the case of the dental clinic, plans include partial maxillofacial service and digitalization of reservations and services, to which the Foundation may cooperate. The area where the Center is located includes a Municipal School for the primary, basic and Bachelor levels, a small observatory and a football field. The total expenditure sustained by the municipality for the operation of the center in 2019 (January-August) amounted to ca 1,400, 000 Quetzals (ca. 200,000 USD). During the same period, the fees charged to the patients were suspended in consideration of the extremely poor level of most of the population.
Fernandez did not run for a second term. A new Mayor, of the same group, elected in July 2019, shall take office in January 2020.
San Juan Alotenango
The third clinic, designed as a two-party venture between the Foundation and the Municipality of San Juan Alotenango, was planned to begin operations in the municipal building in late 2012, under the administration of the Mayor Luis Jose Marroquin. The project was however terminated days before the inauguration. Decisions inconsistent with the By-Laws were unilaterally taken by the Municipality, particularly the selection of a student (EPS) in place of a professional doctor as required by the By-Laws. The Municipality was invited to reconsider their decisions and urgently call the first meeting of the board. The Municipality did not comply with the requirement of the Foundation and the equipment purchased by the Foundation was later transferred to the Municipal clinic of Santa Catarina Barahona. Following unsuccessful attempt to establish a Municipal Clinic, the Municipality favored the establishment of a private clinic. Being the only private dental care center in a relatively large town, the clinic experiences a situation of large demand and reduced competition. However, the local Centro de Salud of the public health service has long been hosting a small dental clinic. The latter currently provides free services offered by an experienced dentist assisted by a nurse. School children are attended from Monday until Thursday (8:00 to 12:00) and adult patients are attended on Fridays. A new building hosting the Centro de Salud has recently been built in Alotenango with increased medical facilities, but is not yet operative. A new administration replaced the Marroquin administration in January 2020.
Conclusions
The excellent results obtained by the clinics in the Santa Catarina Barahona and in San Miguel Dueñas suggest that an increased cooperation between municipalities and private foundations is a viable approach for providing adequate medical care in rural areas of Guatemala without repelling the free medical care law. The continuity of the same Administration over a decade contributed to the success of the clinic in Santa Catarina. In the case of Dueñas, a change in the Municipal Administration did occur, but resulted in in an expansion of municipal care to other areas of medicine. Charges imposed to patients were particularly low in Santa Catarina, and totally can curtailed in Dueñas. In both cases, the actual contribution of the private foundation is being gradually reduced and the municipal clinics are attaining the role of the main supporters of medical care. In the case of Alotenango, however, any attempt to establish a synergy between the municipality and a private foundation failed, and a private, clinic has taken hold the relatively large size of the population has allowed the establishment of a Centro de Salud of the Public Health Service, thus mitigating the lack of municipal involvement. The possibility that the functioning of the municipal clinics might be curtailed by changes in the municipal policies should definitively be considered. The population of the town, the Foundation and the Ministry of Health have stakes in the clinics and ought to be involved in assuring their stability. In The following strategies have been suggested to the Ministry of Health2.
- The population ought to be made aware that the clinics are a permanent asset of the town, resisting any attempt to curtail services, moving the clinic or hiring non-experienced personnel.
- The text of the bilateral agreement should be legalized, and the Foundation should be adamantine in requesting the respect of by-laws.
- The Ministry of Health should issue a quality certification and verify performance on a regular basis.
The data in Tables 2 and 3 evidence the increase of the earning/expenditure ratio with the number of patients and with the individual charges they pay. Therefore, monopolistic situations need to be prevented. The size of the town should define the critical parameter for the prevalence of the public health institutions.
The interplay of the public and the private sectors in the health scare has been a matter of debate in several nations. Some European countries had to completely overhaul their free health care systems in relatively recent times and have now reached the top of a WHF quality classification. Determining factors have been the adoption of limited charges for the services provided, the increase of salaries for doctors and efficient management. Lack of resources prevents the adoption of similar strategies in Guatemala. However, Guatemala could expand on a larger scale the synergic cooperation between private non-profit agencies and municipalities. This approach might facilitate an increase of resources to the larger institutions of the public health service. It would also generate a participation of local initiatives and resources that a centralized system could not easily stimulate. The p direct work of non-profit private care centers, such as the Asociation Obras Sociales del Santo Hermano Pedro and the Rekko clinic, should also allow freeing of additional resources for the public system.
References:
1 Código de Salud Nuevo 1997 Organismo Legislativo Congreso de la República de Guatemala Decreto Nº 90 - 97.
2Letter addressed to the Ministry of Health in the Foundation (see 2015 archive).